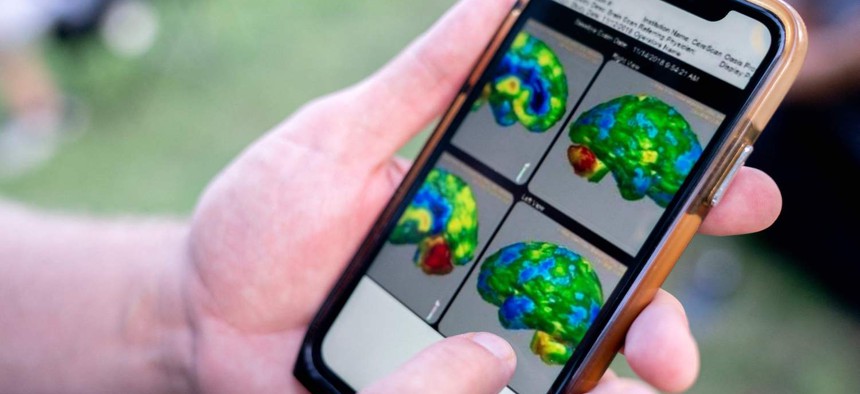
Kevin Hensley, an Iraq and Afghanistan war veteran from Michigan, shows brain scans from medical procedures he had done, outside the U.S. Capitol in Washington, DC, on August 1, 2022. Green represents portions of the brain affected by toxic brain injury, blue represents traumatic brain injury, yellow represents anxiety and depression, and red represents post traumatic stress. STEFANI REYNOLDS / AFP via Getty Images
When will the Pentagon listen on blast injuries?
Troops buffeted by explosions are too often treated simply for mental health—not physical damage to the brain.
The autopsy of Robert Card, who killed 18 people and wounded 13 more in a rampage in Maine last fall, reported severe damage in his brain—scarring, inflammation, damaged tissue, missing white matter. The injuries likely contributed to his erratic and paranoid behavior leading up to the October mass shooting. And it was almost certainly his military service — which included years as a grenade instructor—that led to his injuries.
What happened to Card during his time in the military represents a common scenario: a service member gets exposed to countless low-level blasts, such as from throwing grenades, firing cannons, or breaching walls. They report symptoms such as cognitive impairment, sleep disturbances, panic attacks, depression, and/or memory problems. Then they are diagnosed with a mental health or psychiatric condition and prescribed a cocktail of medications, many of which come with awful side effects.
This default—that the problem is one of mental health—has dominated the treatment of those in uniform since the “shell-shocked” soldiers of World War I. But how much of what we’re seeing in terms of PTSD and even veteran suicide is in fact the result of injury to the brain?
The Pentagon currently requires service members to take individual responsibility for monitoring, reporting, and reducing their own exposure to blasts—an approach that has, at best, a moderate level of feasibility. Symptoms of brain injury from low-level blasts might appear weeks, months, even years after exposure. They can also easily be confused with effects of other service-related injuries.
Even among soldiers who recognized that they’ve suffered a possible head or brain injury, only half sought medical care for a slew of reasons, including worries about hurting their military careers.
Over the past two decades, the Defense Department has made several attempts to better track and prevent these injuries, with lackluster results. It has issued guidance on shooting limits, tried out blast gauges worn by soldiers, proposed improved hearing protection. But efforts have been inconsistent or just partial fixes. Emerging technologies such as implantable sensors to detect early signs of injury are neither mature enough nor practical for the battlefield.
Studies also show that there’s inconsistent awareness and compliance with the safety guidelines that do exist.
Historically, the Pentagon has been slow to implement changes to protect service members from environmental risks. As early as 1957, internal Dow Chemical Company reports suggest that the military was aware that Agent Orange had potentially carcinogenic effects, and yet it was used extensively during the Vietnam War from 1962-69. Since the first Gulf War, the toxic fumes from open-air incineration sites commonly called “burn pits” have been linked to respiratory illnesses since at least 2008. In 2019, at least nine burn pits were still in operation. An estimated 3.5 million troops have suffered health consequences.
In this case, the environmental effect isn’t chemicals or fumes, but damaging overpressure from explosions. The damage discovered in Mr. Card’s brain is by no stretch a singular event. Nearly half a million service members sustained a traumatic brain injury from 2000 to 2023 and countless more may have experienced sub-concussive, or microscopic, brain injuries with disastrous results, as investigative journalists are beginning to reveal. Post-mortem examinations have found brain injuries to service members in the areas responsible for decision-making, memory, and reasoning. These reports should act as a warning, but it seems the Defense Department isn’t responding to the research.
Nor is it listening to bipartisan pleas from Congress. Just last month at a Senate Armed Services Committee hearing, multiple people from inside and outside the Pentagon testified that progress isn’t being made quickly enough and people are dying as a result. The United States has hundreds of thousands of veterans using the VA to help treat their traumatic brain injuries. It has a crisis of suicides among service members and veterans driven by inadequate screening for brain injuries. And now it has 31 civilians dead and injured in Maine.
The Pentagon’s response continues to be that it needs more research, more tools, more time. But it’s clear that the research is pointing to brain injuries as a major health problem, in the military and elsewhere. More tools might help the military identify cases, but they won't accomplish the essential: drastically cutting the exposure to blasts. As for time, the Pentagon has had plenty.
Samantha McBirney is a biomedical engineer who has studied traumatic brain injury from blunt impact and blast overpressure for 15 years at RAND, UC Berkeley, and the University of Southern California. Emily Hoch is a senior policy analyst at RAND, where she and McBirney lead research on the health impacts of blast injuries to service members.
NEXT STORY: Should governments ban TikTok? Can they?